Question 7 of 8
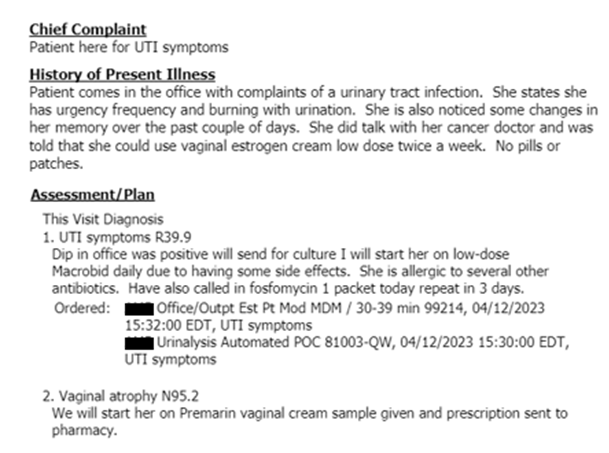
6. Urogynecology record. Reviewing this record and the corresponding claim record (what was billed) do you agree or disagree and what codes would you assign for the encounter visit and the diagnosis?
Claim info:

Record documentation: (answer question based on this documentation alone)
Select the best answer from below.